Constant Severe Anal Pain? Long-Term Anal Fissure Treatment in Hadapsar Pune That Actually Works
- Home
- Anorectal Surgery
- Constant Severe Anal Pain? Long-Term Anal Fissure Treatment in Hadapsar Pune That Actually Works
Constant Severe Anal Pain? Long-Term Anal Fissure Treatment in Hadapsar Pune That Actually Works
📌 Quick Treatment Guide — Anal Fissure Treatment in Hadapsar Pune
Q: What is an anal fissure?
A small tear in the lining of the anal canal that causes sharp, burning pain during and after bowel movements. It is different from piles. Chronic fissures persist beyond 6–8 weeks and require specialist care.
Q: Is Anal Fissure Treatment in Hadapsar Pune available without major surgery?
No. Dr. Mangesh Yadav offers modern laser-assisted fissure treatment — a daycare procedure with no large incision, minimal pain, and same-day discharge. Open surgery is rarely needed today.
Q: When should I see an Anorectal surgery specialist in Hadapsar?
Immediately if pain has lasted more than 4–6 weeks, if creams have stopped working, or if you see a visible skin tag or sentinel pile near the tear. Delaying worsens sphincter tightness.
Q: Can a chronic anal fissure heal without surgery?
Rarely. Acute fissures can heal with diet and topical medication. Chronic fissures with a hypertonic sphincter almost always need clinical intervention — botox injection or laser sphincterotomy.
Q: How does laser fissure repair prevent recurrence?
Laser precisely relaxes the internal sphincter, eliminating the root cause of poor blood supply and spasm. This promotes complete tissue healing and dramatically reduces the chance of the fissure returning.
Anal Fissure Treatment in Hadapsar Pune is something many patients desperately need but hesitate to seek — and that hesitation only makes the problem worse. If you have been dealing with a burning, tearing sensation every time you use the toilet, if you dread the morning because you know what is coming, and if over-the-counter creams have stopped offering any real relief, you are not alone. Thousands of patients in Pune quietly suffer from chronic anal fissures — and most of them had no idea that a simple, modern, near-painless solution existed just around the corner.
This guide has been written by Dr. Mangesh Yadav, a trusted General and Anorectal Surgery specialist based in Hadapsar, Pune, to help you understand exactly what is happening inside your body, why the pain keeps coming back, and what today’s most advanced treatment options can do for you — quickly, confidently, and with complete dignity.
Fissure or Piles? Why Misdiagnosis Delays Your Recovery
One of the most common reasons patients delay proper care is a misidentification of their condition. Both fissures and piles involve discomfort in the same region, and both can cause minor bleeding — which leads to enormous confusion. Many patients self-treat with anti-haemorrhoidal ointments for months, only to find that their pain not only persists but worsens.
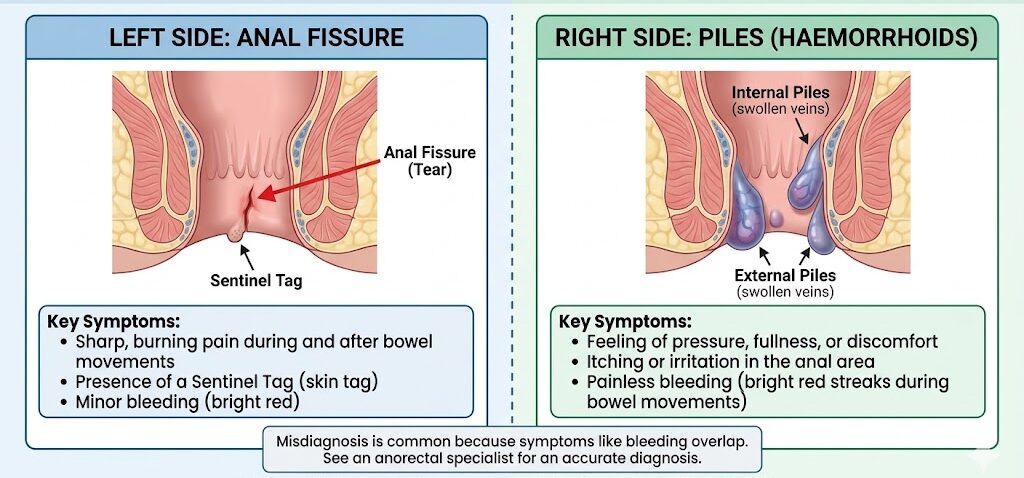
Here is a clear way to understand the distinction. When you sit down for a bowel movement and experience a sharp, burning, tearing pain — one that may linger for 30 minutes to 2 hours afterwards — that is the signature of a fissure. A fissure is a physical crack in the delicate skin lining the anal passage. Piles, by contrast, tend to feel more like pressure, heaviness, wetness, or itching, and the bleeding is usually brighter red and painless.
| Feature | Anal Fissure | Piles (Haemorrhoids) |
|---|---|---|
| Nature | Tear / cut in anal skin | Swollen blood vessels |
| Pain character | Sharp, burning, prolonged | Pressure, dull ache |
| Bleeding | Small amount, bright red | Dripping / streaks, bright red |
| Duration of pain | 30 min – 2 hrs post-stool | During defecation only |
| Visible sign | Sentinel skin tag at base | External lump or prolapse |
| Root cause | Sphincter spasm / poor blood supply | Venous engorgement |
Getting this distinction right is the first step. A proper clinical examination by an Anorectal surgery specialist in Hadapsar takes only a few minutes and saves you months of ineffective self-treatment. At Dr. Mangesh Yadav’s clinic, every consultation begins with a thorough, gentle, and completely confidential examination — because accurate diagnosis is the foundation of effective care.
What Causes Chronic Painful Tears That Demand Specialized Anal Fissure Treatment in Hadapsar Pune?
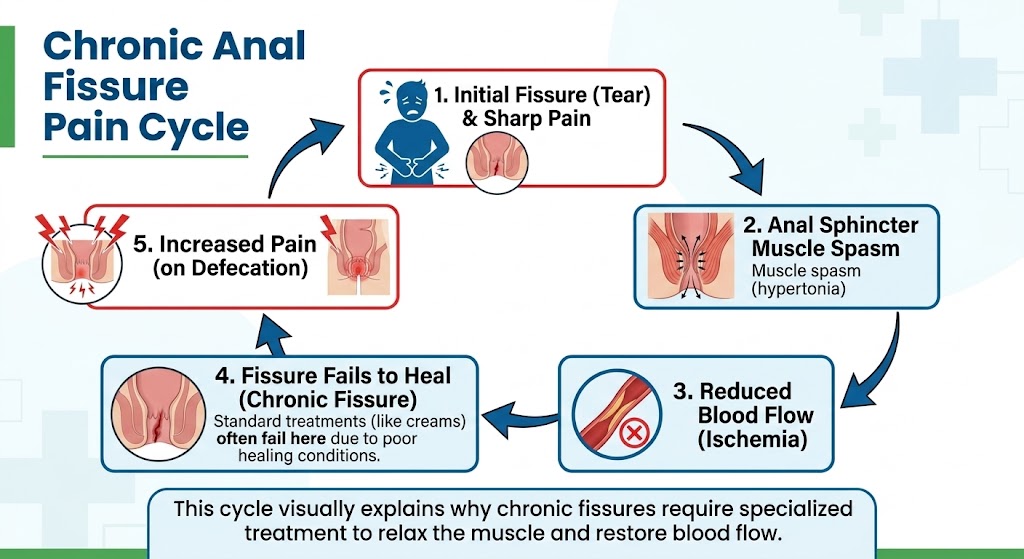
Anal fissures begin simply. Hard stools, constipation, sudden diarrhoea, or trauma during childbirth can create an initial small tear in the anal canal. In most cases, with a little dietary correction and a sitz bath routine, this heals within a week or two. But when the body’s natural healing response is blocked — that is when a fissure becomes chronic.
The key culprit is the internal anal sphincter muscle. When a fissure is present, the body instinctively tightens this muscle to protect the area from pain. Unfortunately, this tightening (called sphincter hypertonia) compresses the tiny blood vessels that should be delivering oxygen and nutrients to heal the wound. Without blood supply, the wound cannot heal. The pain from the wound causes more tightening. More tightening means less blood. Less blood means no healing. This cycle repeats itself, day after painful day.
Common Risk Factors
- Chronic constipation and repeated straining at stool
- Low-fibre diet common in urban Indian households
- Dehydration — a very common trigger in Pune’s summer months
- Childbirth trauma, especially after difficult or prolonged labour
- Sedentary lifestyle with prolonged sitting (office workers, drivers)
- Inflammatory bowel conditions like Crohn’s disease
- Previous anorectal procedures that left scar tissue
Many patients in Hadapsar and the wider Pune region also present with what is called a sentinel pile — a small, fleshy skin tag at the outer edge of the fissure. This is a tell-tale sign that the fissure has become chronic. It is not a separate condition; it is the body’s scar response to a wound that keeps reopening. When this tag is present, dietary measures alone are almost never enough.
When You Must Not Wait Any Longer
If your fissure pain has been present for more than 6 weeks, if you are avoiding meals to avoid the pain of defecation, or if you notice a visible lump or skin tag near the tear — please do not delay. Untreated chronic fissures can worsen sphincter fibrosis, making future treatment more complex than it needs to be. Early intervention means easier recovery.
When Does an Anorectal Surgery Specialist in Hadapsar Advise Clinical Sphincterotomy Over High-Fibre Diets?
This is the question most patients are afraid to ask — and the answer is refreshingly straightforward. The goal is always to cure the fissure with the least invasive approach possible. Dr. Mangesh Yadav follows a structured treatment ladder that begins gently and escalates only when necessary.
Step 1: Conservative Management (Weeks 1–6)
- High-fibre diet (25–35 g/day) and adequate hydration
- Warm sitz baths 2–3 times daily to relax the sphincter
- Topical nitroglycerine or diltiazem ointment to improve blood flow
- Stool softeners to prevent straining
This conservative phase works well for acute fissures. However, studies consistently show that roughly 40–50% of chronic fissures fail to respond to these measures alone — particularly when the internal sphincter has been in spasm for weeks or months.
Step 2: Botulinum Toxin (Botox) Injection
When topical measures fail, Dr. Mangesh Yadav may recommend a Botox injection into the internal sphincter. This is a quick, near-painless office procedure that temporarily relaxes the sphincter for 3–4 months, giving the fissure time to heal. It works in approximately 70–80% of chronic cases and requires no hospitalisation.
Modern laser-assisted sphincterotomy for chronic anal fissure — performed by Dr. Mangesh Yadav, Anorectal surgery specialist in Hadapsar, Pune.
Step 3: Lateral Internal Sphincterotomy (LIS)
For patients in whom Botox does not provide lasting relief, or who have significant sphincter fibrosis, Lateral Internal Sphincterotomy (LIS) is the gold-standard surgical option. This procedure involves making a precise, controlled division of a small portion of the internal sphincter muscle — permanently relieving the excessive tension that prevents healing.
Performed with laser precision today, this is no longer the intimidating operation it once was. At Dr. Mangesh Yadav’s practice, it is done as a daycare procedure under short anaesthesia. Patients walk out the same day, experience significant pain relief within 48–72 hours, and return to normal life within a week.
How Do Laser Fissure Repairs Prevent Future Recurrences and Ensure Rapid Tissue Healing?
The word “laser” can sound alarming to patients who are already anxious about a sensitive procedure. The reality is the opposite — laser-assisted anorectal surgery is gentler, faster, and more precise than conventional open techniques. And for chronic anal fissure specifically, it has transformed patient outcomes in ways that were not possible even ten years ago.
What Happens During a Laser Fissure Procedure?
- Pre-procedure assessment: A short clinical examination confirms the fissure’s location, depth, and whether a sentinel pile or skin tag is present. This takes less than five minutes.
- Anaesthesia: The patient receives short-acting local or spinal anaesthesia. There is no awareness of the procedure itself.
- Laser sphincterotomy: A thin laser probe is introduced. The laser energy precisely and selectively cuts a small portion of the internal sphincter, immediately reducing its resting pressure — and therefore restoring blood supply to the fissure bed.
- Wound treatment: If a sentinel pile or skin tag is present, it is removed simultaneously. The wound is small and heals rapidly.
- Recovery and discharge: The patient rests for 2–3 hours and is discharged the same day with simple post-procedure instructions.
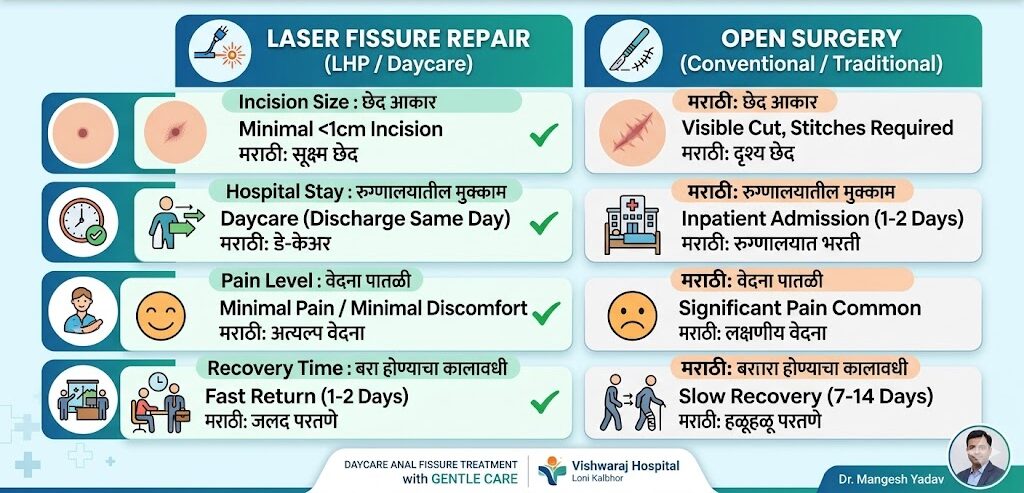
Laser vs. Open Surgery — Why Laser Wins
| Parameter | Laser Sphincterotomy | Conventional Open Surgery |
|---|---|---|
| Incision size | Minimal (sub-cm) | Larger wound |
| Bleeding | Near zero | More, with packing needed |
| Hospital stay | Same-day discharge | 1–2 days admission |
| Post-op pain | Mild and brief | Significant, longer duration |
| Return to work | 5–7 days | 10–14 days |
| Recurrence risk | Very low (<5%) | Slightly higher |
| Risk of incontinence | Extremely low with precision | Slightly higher |
The precision of laser energy means that only the targeted portion of the sphincter is addressed. Surrounding healthy tissue is entirely preserved. This is what makes recurrence rates so low — the procedure corrects the mechanical root cause rather than simply managing the surface wound.
Why Patients Choose Dr. Mangesh Yadav for Anorectal Care — Dignity, Confidentiality, and Expertise
We understand that conditions affecting the anal and rectal area carry an emotional weight that most other health concerns do not. The embarrassment, the hesitation, the fear of being judged — these are real feelings that prevent thousands of people from getting care they genuinely need. And every day without treatment, the fissure deepens, the sphincter tightens further, and the pain compounds.
At Dr. Mangesh Yadav’s clinic at Vishwaraj Hospital, you will be treated exactly as you deserve — as a patient who is seeking help for a medical condition, with no different treatment than someone walking in for a thyroid check or a knee pain consultation. The examination room is private. Your diagnosis is never shared. Your file is handled with complete confidentiality.
Dr. Mangesh Yadav, MS in General Surgery, has extensive experience with anorectal disorders including fissures, fistulas, piles, and complex rectal conditions. His approach is simple: explain everything clearly, treat conservatively where possible, and use surgical precision only when it delivers you a permanent solution. You will never be rushed into a procedure, and you will never be left without answers.
The Risks of Delaying Anal Fissure Treatment — Why "Waiting It Out" Makes Things Worse
One of the most damaging things a patient with a chronic fissure can do is wait. This is not impatience on the doctor’s part — it is a clinical reality. The longer the internal sphincter remains in a state of hypertonia, the more fibrotic (scar-like) it becomes. Fibrotic sphincter tissue is harder to relax with medication, may respond poorly to Botox, and ultimately may require a more extensive surgical correction.
Beyond the sphincter itself, chronic fissure pain modifies behaviour in ways that create secondary health problems. Patients begin avoiding certain foods or reducing meal frequency to minimise bowel movements. This leads to constipation — which ironically worsens the very fissure they are trying to protect. Some patients stop walking or exercising, leading to further bowel slowing. The cycle becomes entrenched.
The decision to see a specialist is not a decision to “go under the knife.” It is a decision to get an accurate diagnosis, understand your options, and start a treatment path that may be as simple as a dietary overhaul and a medicated cream — or may need a 20-minute laser procedure that solves the problem permanently. Either way, the information from that consultation is invaluable.
For further reference on anorectal health and fissure management guidelines, the American Society of Colon and Rectal Surgeons (FASCRS) offers comprehensive, evidence-based patient resources.
Recovery After Laser Anal Fissure Surgery — What to Expect Week by Week
Your Recovery Timeline
- Day 1–2 (Rest at home): Mild soreness is normal. Warm sitz baths 2–3 times daily. Light, fibre-rich meals. Take prescribed analgesics as needed.
- Day 3–5 (Noticeable improvement): Most patients report that the burning post-stool pain — the most distressing symptom — has reduced by 60–80%. Movement and walking are encouraged.
- Day 5–7 (Return to routine): Office work and light daily activities can resume. Avoid heavy lifting or strenuous exercise for another week.
- Week 2–4 (Progressive healing): The small wound from the procedure continues to heal. Continue sitz baths. Follow-up visit with Dr. Mangesh Yadav to assess healing progress.
- Week 4–6 (Complete healing): The fissure site is fully healed in the vast majority of patients. Long-term dietary habits (high fibre, adequate water) are reinforced to prevent any future fissures.
Frequently Asked Questions
What is an anal fissure and how is it different from piles?
An anal fissure is a small tear in the anal canal lining that causes sharp, burning pain during and after passing stool. Piles are swollen blood vessels that cause bleeding, itching, or a lump. These are two different conditions requiring different treatments — a specialist can confirm the exact diagnosis in one gentle examination.
What are the main causes of chronic anal fissure that don't heal on their own?
How do I know if my anal fissure has become chronic?
If your anal pain has lasted more than 6–8 weeks despite using ointments and dietary changes, your fissure is likely chronic. Other signs include a visible skin tag or sentinel pile near the tear, extreme pain after every bowel movement lasting 30 minutes or more, and bleeding that does not reduce.
Is Anal Fissure Treatment in Hadapsar Pune available without major surgery?
Yes. Dr. Mangesh Yadav offers modern laser-assisted fissure treatment — a daycare procedure with no large incision, minimal bleeding, and same-day discharge. Most chronic fissures are resolved with Botox injection or laser sphincterotomy. Open surgery is rarely needed with today’s techniques.
When does an Anorectal surgery specialist in Hadapsar recommend sphincterotomy?
Is laser fissure treatment painful? What happens during the procedure?
No — the procedure is performed under short anaesthesia and is completely painless. A laser probe precisely relaxes a small portion of the tight sphincter muscle, restoring blood supply to the wound. The entire procedure takes 20–30 minutes. Patients rest for 2–3 hours and go home the same day.
How does laser fissure repair prevent future recurrences?
Laser treatment eliminates the root cause — the hypertonic (over-tight) sphincter muscle — rather than just managing the surface wound. By restoring normal blood flow to the anal canal, the tissue heals completely. Recurrence after laser sphincterotomy is under 5%, far lower than with ointments alone.
How long is recovery after anal fissure laser surgery in Pune?
Most patients feel 60–80% pain relief within 48–72 hours. They return to desk work in 5–7 days. Full tissue healing takes 4–6 weeks. Warm sitz baths 2–3 times daily, a high-fibre diet, and adequate water intake are the only post-procedure requirements.
Is the consultation for anal fissure completely confidential at Dr. Mangesh Yadav's clinic?
Yes — absolutely. All anorectal consultations at Dr. Mangesh Yadav’s clinic at Vishwaraj Hospital, Hadapsar are conducted with complete privacy and dignity. Your diagnosis is never shared. The examination is gentle, and every patient is treated with the same respect as any other medical concern.
Ready to End the Pain — For Good?
You deserve to eat, walk, and live without dreading the bathroom. A confidential consultation with Dr. Mangesh Yadav takes 15 minutes and gives you a complete roadmap to lasting relief. No judgment. No rush. Just clear answers and expert care.
Book your private consultation today. Confidential. Comfortable. Permanent.
Vishwaraj Hospital, Pune Solapur Road, Loni Kalbhor, Pune 412201 +91-8220131599 | +91-9653331571
Disclaimer: This blog is for informational purposes only. Please consult Dr. Mangesh Yadav for personalised diagnosis and treatment recommendations.
Need Help? We’ve Got You Covered
Contact Details
Clinic Address
153, Magarpatta Rd, Magarpatta, Hadapsar, Pune
Monday To Saturday: 03.00 PM to 05.00 PM / 07.00 PM to 08.30 PM
Sunday: 10.30 AM to 01.00 PM